Electrical
injury may cause various ocular complications without major damage to other
organs of the body. Electrical voltage ranging from 220 to 50 000, can lead to
cataract formation in 5% to 20% of cases.1 A detailed ocular
examination should be performed at presentation or as soon as practical for
documentation. The final visual outcome after cataract surgery depends on other
ocular complications caused by electric current2. We report a case
of electrical injury induced cataract with other ocular complications
developing after exposure to electric current.
CASE REPORT
A 60 years old male complained of painless progressive diminution
of vision in both eyes for the preceding 1 month. There was history of
unconsciousness with burn of scalp, face, back and legs following high voltage
electrical injury (12000 volts) about two months back for which he was admitted
in hospital and was treated conservatively.
Ocular examination revealed visual acuity of perception of light
(PL + VE) with accurate projection of rays in both eyes. There was ciliary congestion and sluggishly reacting pupil in both
eyes (BE) with anisocoria. Slit lamp examination
revealed advanced immature cataract in BE (Fig. 1). Left eye (LE) pupil was
irregular with posterior synechiae extending from
9-12 0’clock. The intraocular pressure was 21 mm Hg in both eyes. The posterior
segment was normal on B – scan ultrasonography in both eyes. General physical
examination showed non-healing scalp wound which was about 10 cm × 4 cm in size
(Fig. 2). Face, back and legs showed healed lesion of burn injury.
On the
basis of history and clinical examination a diagnosis of bilateral electric
cataract with anisocoria and resolving iritis was made. Patient underwent small incision cataract
surgery with posterior chamber intraocular lens implantation in BE at an
interval of one week. Postoperatively corrected visual acuity was 6/24 in right
eye and 6/60 in left eye. Fundus examination revealed marked pallor of the disc
(LE > RE) with normal cup: disc ratio (Fig. 3). Macula showed dull
reflex in BE with retinal pigment epithelial defects. Fundus flurescein angiography was within normal limit.
DISCUSSION
Ocular
complications from electrical burn injuries are not very common. Anterior
segment involvement in the form of corneal burn, anisocoria,
acute bilateral iritis has been reported. Posterior
segment complications like vitreous hemorrhage or vascular occlusion, retinal
detachment, macular cyst, macular hole, optic
neuropathy, papillopathy, papilledema, optic atrophy
has been reported.3

Fig. 1: Bilateral electric cataract with posterior synechiae
in the left eye

Fig.2: Electrical injury induced non-healing scalp wound.
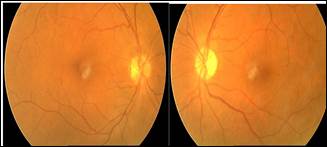
Fig. 3: Bilateral disc pallor.
The anterior segment complications are considered to be due to
secondary to heat, as well as electrical injury. Posterior segment changes are
thought to be caused by the passage of electrical current.4
Lenticular opacities following electrical trauma usually occur
with a latency period varying from immediately after injury to a few years.5
The closer the point of contact of the current to the eye, the greater
the chance of cataract formation. The crystalline lens is a good conductor of
electric current because of its high water content. Electrical injury seems to
change the capsular permeability directly or indirectly6. Typical
electric cataract starts as snowflake-like anterior subcapsular
lens opacities which we missed, as our case presented with advanced stage of
cataract. Bouzalis DT et al reviewed one hundred
fifty- nine patients with high voltage electrical injuries, out of which two
had recurrent iritis, eight had cataracts, two had
macular holes, and one had central retinal artery occlusion.7
In our
case, we presume that bilateral cataract, iritis,
optic atrophy was all caused by high voltage electrical current (12,000 volt).
Poor visual recovery post operatively is related to optic neuropathy induced by
electrical injury. Most of the ocular changes occur immediately after injury,
but some late changes may also occur days to years after a severe electrical
injury. High - voltage injury patients usually present with severe burns
requiring prolonged hospitalization. Referral to an ophthalmologist and careful
follow-up is recommended in all cases of ocular / scalp electrical injuries.
Author’s Affiliation
Dr. Chandana Chakraborti
Assistant Professor
A/1/1, Pearl Apartment
50B, Kailas Bose Street, Kolkata 700006
Dr. Swati Mazumder
Assistant Professor
Department of Ophthalmology
Maldah Medical College
West Bengal
REFERENCES
1.
Johnson EV, Kline LB, Skalka HW. Electrical cataracts: A case report and review of literature.
Ophthalmic Surg.1987; 18: 283-5.
2.
Biro
Z, Pamer Z. Electrical cataract and
optic neuropathy. Int Ophthalmol. 1994; 18: 43–7.
3.
Robert E, Raymond M, Paul F. Electrical injuries: Engineering, medical and legal aspects. 2nd
ed. Lawyers Judges publishing company, 2004: 401.
4.
Bienfang DC, Zakov ZN, Albert DM. Severe electrical burn of the eye. Graefe’s
Archive for Clinical and Experimental Ophthalmology. 1980; 214: 147-3.
5.
Hanna C, Fraunfelder FT. Electric cataracts. II: Ultrastructural
lens changes. Arch Ophthalmol.1972; 87: 184-91.
6.
Grewal DS,
Jain R, Brar GS, Grewal
SPS. Unilateral electric cataract: Scheimpflug imaging and review of the literature. J
Cataract Refract Surg. 2007; 33: 116-9.
7.
Boozalis
GT, Purdue GF, McCulley JP. Ocular changes from electrical burn
injuries: A literature review and report of cases. J Burn Care Rehabil. 1991; 12: 458-2.